A 22-year-old man collapsed from dehydration during maneuvers in the desert and was sent to an emergency. A high level of glucose was observed in his urine. He was suspected of being a diabetic. Further tests, however, determined that his serum insulin level was normal. A glucose tolerance test exhibited a normal pattern; further testing of the urine revealed that only D-glucose was elevated. Other sugars were not elevated. The patient was diagnosed with, ‘Renal glycosuria’. This patient’s elevated urinary glucose and his dehydration episode are caused by a deficiency in which of the following?
A. GLUT 2
B. GLUT 4
C. Insulin receptor
D. SGLT1
E. SGLT2
The correct answer is E- SGLT2.
The patient has impaired reabsorption of glucose from the tubular filtrate, an absorption defect due to deficiency of SGLT2 (sodium-dependent glucose transporter-2).
Since blood glucose is normal; the glucose tolerance test is also normal, the possibility of diabetes mellitus is ruled out. Renal glycosuria in the current situation is due to the excessive excretion of glucose in urine. Glucose absorption across the intestinal and renal tubular cells is an active transport (against the concentration gradient, requiring energy and a carrier protein). It is a co-transport; sodium is also transported by the carrier protein. Sodium moves down the concentration gradient while the movement of glucose is against the concentration gradient.
SGLT-1 is mainly a transporter of glucose in Intestinal cells (luminal surface), deficiency of which causes impaired absorption of dietary glucose.
SGLT-2 is a sodium-dependent glucose transporter in the proximal renal tubules. 90 percent of filtered glucose is reabsorbed through SGLT-2, the deficiency of which causes renal glycosuria, as in the present situation. SGLT-2 inhibitors are used in the treatment of Diabetes mellitus. Sodium-glucose co-transporter 2 (SGLT2) inhibitors, also known as gliflozin drugs, are a new class of diabetic medications indicated for the treatment of type 2 diabetes. SGLT2 inhibitors block the reabsorption of glucose in the kidney, increase glucose excretion, and lower blood glucose levels (figure).
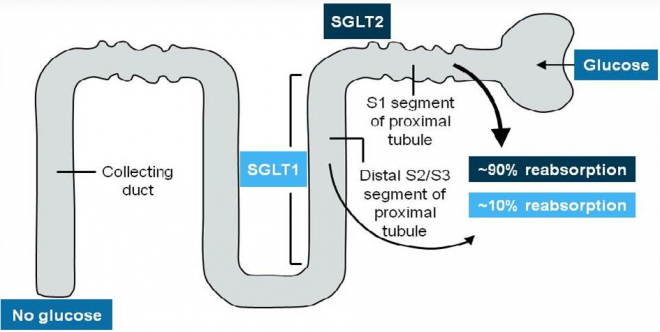
Figure-showing the mechanism of action of SGLT-2 (source-http://www.diabetesincontrol.com/sglt2-inhibitors-a-new-class-of-diabetes-medications/)
GLUT 2 and GLUT4 are sodium independent glucose transporters,
GLUT2 is present in liver and pancreatic beta cells, whereas GLUT-4 is present in adipose tissue and skeletal muscle. This is the only glucose transporter that is under the control of Insulin. Insulin promotes the uptake of glucose by muscle and fat.
The insulin receptor is not involved in the reabsorption of glucose from the tubular filtrate