
Search Your Topic
Heparin- Mechanism of action-a case study
Case Details
A 54 –year- old woman who was bed-bound in a nursing home began to develop swelling of her left leg. She was evaluated with venous Doppler ultrasound and was found to have a deep vein thrombosis. She was immediately started on heparin to prevent the clot from further enlarging.
What is the chemical nature of Heparin?
How will it help in preventing clot formation?
Case discussion
Heparin
Heparin also called α Heparin, is a highly sulfated GAG(Glycosaminoglycans). It is an anticoagulant widely used in clinical practice. It is present in the liver, lungs, spleen, and monocytes. Commercial preparations are from animal lung tissues. It contains repeating units of sulfated Glucosamine and either of the two uronic acids-D-Glucuronic acid and L-Iduronic acid. In fully formed Heparin molecules 90% or more of uronic acid residues is L-Iduronic acid. It is strongly acidic due to sulphuric acid groups and readily forms salts.
Clinical role of Heparin
In vitro Heparin is used as an anticoagulant while taking blood samples, 2 mg/10 ml of blood is used. It is considered the most satisfactory anticoagulant as it does not produce a change in red cell volume or interfere with subsequent determinations.
In vivo, Heparin is used in suspected thromboembolic conditions to prevent intravascular coagulation. Heparin is used for anticoagulation for the following conditions:
- Acute coronary syndrome,
- Atrial fibrillation
- Deep-vein thrombosis and pulmonary embolism.
- Cardiopulmonary bypass for heart surgery.
Mechanism of action
Role of heparin as an anti-coagulant
It produces its major anticoagulant effect by inactivating thrombin and activated factor X (factor Xa) through an antithrombin (AT) dependent mechanism. Heparin binds to AT through a high-affinity pentasaccharide. (See figure-1)
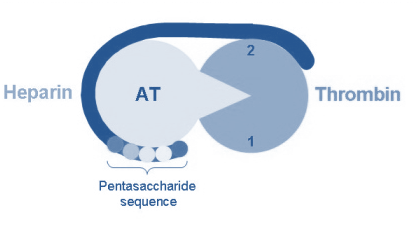

Figure-1-showing the binding of heparin to antithrombin. To potentiate thrombin inhibition, heparin must simultaneously bind to antithrombin and thrombin.
Binding of Heparin to lysine residues in antithrombin produces conformational changes that promote the binding of the latter to serine protease “thrombin” which is inhibited, thus fibrinogen is not converted to fibrin and the coagulation is inhibited (figure -2).


Figure-2-showing the mechanism of action of Heparin. Heparin has a multitude of effects on the clotting cascade; however, the primary sites of action are the inhibition of factor II, also called thrombin and factor X.
Role of Heparin as a coenzyme
Heparin acts in the body to potentiate the activity of the enzyme “Lipoprotein lipase”. Heparin binds specifically to the enzyme present in capillary walls causing its release into the circulation. Hence it is also called “releasing factor”.
Administration of Heparin
Heparin is given parenterally, as it is degraded when taken by mouth. It can be injected intravenously or subcutaneously. Intramuscular injections are avoided because of the potential for forming hematomas.
Because of its short biologic half-life of approximately one hour, heparin must be given frequently or as a continuous infusion. However, the use of low-molecular-weight heparin (LMWH) has allowed once-daily dosing, thus not requiring a continuous infusion of the drug. If long-term anticoagulation is required, heparin is often used only to commence anticoagulation therapy until the oral anticoagulant Warfarin takes effect.
Adverse effects
The most common side effect is bleeding. The risk of bleeding increases with a higher dosage.
A serious side-effect of heparin is heparin-induced thrombocytopenia (HIT). HIT is caused by an immunological reaction that makes platelets a target of immunological response, resulting in the degradation of platelets. This is what causes thrombocytopenia. This condition is usually reversed on discontinuation, and can generally be avoided with the use of synthetic heparins. There is also a benign form of thrombocytopenia associated with early heparin use, which resolves without stopping heparin.
There are two non-hemorrhagic side-effects of heparin treatment. The first is the elevation of serum Aminotransferases levels, which has been reported in as many as 80% of patients receiving heparin. This abnormality is not associated with liver dysfunction, and it disappears after the drug is discontinued. The other complication is hyperkalemia, which occurs in 5 to10% of patients receiving heparin, and is the result of heparin-induced aldosterone suppression. The hyperkalemia can appear within a few days after the onset of heparin therapy.
Osteoporosis – has also been reported with long-term Heparin therapy, since Heparin causes bone loss both by decreasing bone formation and by enhancing bone resorption.
Go ahead.
Thanks