
Search Your Topic
Case study- Luft syndrome (Hypermetabolic mitochondrial syndrome)
Case Study
A 30 -year- old patient reported to medical OPD complaining of generalized weakness, excessive perspiration, and high caloric intake without an increase in body weight. From the age of seven, she had suffered from profuse sweating that forced her to change clothes about ten times a day. To compensate for the loss of fluids she had to drink many liters of water every day. Her calorie intake was about 3500 calories a day, approximately the need for a manual laborer, despite a body weight of only 40 kilograms.
There was no sign of any other disease. The BMR of the patient was excessively elevated but the thyroid hormones (T3 and T4) were in normal concentrations. Laboratory tests showed small deviations from the normal picture, with the exception of her blood volume, which was about twice as large as normal.
What is the probable diagnosis?
Case details The patient is probably suffering from Luft’s syndrome also called Hypermetabolic mitochondrial syndrome.
All the symptoms like high caloric intake but failure to gain weight, excessive perspiration, excessive thirst, etc indicate a state of severe hypermetabolism of non-thyroid origin (since thyroid hormones -T3 and T4 are normal). The defect lies in the maintenance of mitochondrial respiratory control.
Mitochondria play a major role in human energy dynamics (ATP synthesis and related reactions), and a functional deficit may be expected to result in a diminished supply of high energy phosphate bonds. In mitochondria, electron transfer is coupled to oxidative phosphorylation via a proton gradient, and the energy released from oxidation is transferred to the ATP synthase trapping system. A class of compounds called uncouplers can block electron-transfer- linked phosphorylation at any of the three stages (energy production, transfer, or trapping). Redox reactions release free energy (delta G negative), such energy may be dissipated as heat, or be trapped as a proton gradient. Whether energy is dissipated or trapped depends on the characteristics of biologic membranes rather than on the reaction itself. Any substance that allows protons to leak across membranes will play an uncoupling role since it will block the transfer of energy between electron flow and ATP synthesis (figure).
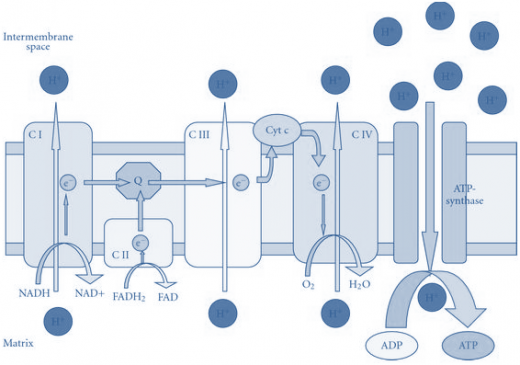
Figure-showing the electro-chemical gradient and the tight coupling between oxidation and phosphorylation in the electron transport chain.
More than 90% of the oxygen used in the human body is utilized by mitochondrial cytochrome oxidase, which transfers four electrons into an oxygen molecule to produce two molecules of water.
Deficits in mitochondrial function arise by two mechanisms: (1) a block in electron flow or ATP synthesis which results in lactic acidosis; and (2)uncoupling electron flow from ATP synthesis (Luft syndrome) in which oxidation occurs at a rapid rate but without a concomitant increase in ATP synthesis (energy released is dissipated as heat).
In Luft syndrome, the uncoupling is caused by an abnormality in the mitochondrial membrane. Electron transport is only loosely coupled to ATP production, thus the extra energy evolves in the form of heat.
Thus this syndrome is characterized by
· Severe hypermetabolism,
· Heat intolerance,
· Profuse perspiration,
· Polyphaga,
· Polydipsia without polyuria,
· Muscular wasting and weakness,
· Absent deep reflexes, and
· Resting tachycardia.
· At the cellular level, the mitochondria respire wildly and waste the excess energy as heat, an elevation of body temperature up to 38.4 °C.
· There is progressive weight loss despite increased food intake.
· The thyroid function is normal.
· Onset is in childhood.
· The rise in BMR is due to the partial uncoupling of oxidative phosphorylation. Since there is less ATP production and the extra energy is lost in the form of heat, all the metabolic processes are stimulated. Due to high BMR only there is a failure to put on weight despite a good diet.
Laboratory Investigations
Routine investigations can be undertaken for differential diagnosis. BMR, Thyroid function tests, blood glucose, etc can be measured to rule out the presence of other conditions with similar symptoms.
Treatment
There is no permanent cure for this disease. Symptomatic treatment can only be given. Vitamin therapy in the form of Vitamins C, K, and E, along with coenzyme Q10 and a high-caloric diet is recommended. Protection from heat is advised.