
Search Your Topic
Case study- Scurvy (vitamin C deficiency)
Case Details
A 4 -year-old boy was brought for consultation for hematuria, edema of lower extremities as well as swollen right leg. He was the 12th born in a poor family, where one previous child died from malnutrition and dehydration in the period of infancy. The child was fed only with cow’s milk and biscuits.
From the period of five months, the boy manifested irritability, sweating, poor appetite and cried when somebody touched him. At admission the baby was afebrile, pale, and malnourished; his hair was dry and cracked. Clinical evaluation showed no organomegaly, no neurological signs, gingival bleeding was there and only one tooth was present.
Laboratory findings were as follows:
- Red Blood Cell Count 3.5 million/mm3
- Hemoglobin (Hb) 7 g/dl
- Hematocrit (Hct) 30%
- Serum Iron low
- Liver function tests were in the normal range.
- The ultrasound of the kidney was normal.
Doppler of blood vessels of both legs was normal which excluded thrombophlebitis. The swelling of the right leg indicated radiological investigation. Massive subperiosteal hematoma on the right femur dilatated metaphyses and general osteoporosis had been present on the radiogram.
What is the probable diagnosis for this child?
Case discussion
The child is most probably suffering from Scurvy (Vitamin C deficiency). As history suggests the child had been an ignored child, fed a diet deficient in fruits and vegetables and the signs and symptoms are also typical of scurvy. Bleeding gums, tooth loss, Subperiosteal hematoma, and bony changes are characteristic of scurvy. Iron deficiency anemia is also there which is very common in scurvy due to various reasons.
Thus considering the osteoskeletal manifestations, malnutrition, anemia, irritability and bleeding tendencies as well as the radiological findings, deficiency of vitamin C is concluded.
Scurvy
Scurvy is a state of dietary deficiency of vitamin C (ascorbic acid). The human body lacks the ability to synthesize vitamin C and therefore depends on exogenous dietary sources to meet vitamin C needs. The enzyme, L-gluconolactone oxidase, which would usually catalyze the conversion of L-gluconolactone to L-ascorbic acid, is defective due to a mutation.
Vitamin C – An overview
Vitamin C (ascorbic acid) plays a role in collagen, carnitine, hormone, and amino acid formation. It is essential for wound healing and facilitates recovery from burns. Vitamin C is also an antioxidant, supports immune function, and facilitates the absorption of iron.
Causes of Vitamin C (Ascorbic Acid) Deficiency
Scurvy is caused by a dietary deficiency of vitamin C. The body’s pool of vitamin C can be depleted in 1-3 months.
- Risk factors include the following:
- Babies who are fed only cow’s milk during the first year of life are at risk.
- Alcoholism and conforming to food fads are risk factors.
- Elderly individuals who eat a tea-and-toast diet are at risk. Retired people who live alone and those who eat primarily fast food face an increased risk of deficiency.
- Economically disadvantaged persons tend to not purchase foods high in vitamin C (eg, green vegetables, citrus fruits), which results in them being at high risk.
- More recently, vitamin C deficiency has been noted in refugees who are dependent on external suppliers for their food and have limited access to fresh fruits and vegetables.
- Cigarette smokers require an increased intake of vitamin C because of lower vitamin C absorption and increased catabolism.
- Pregnant and lactating women and those with thyrotoxicosis require increased intake of vitamin C because of increased utilization.
- People with anorexia nervosa or anorexia from other diseases such as AIDS or cancer are at increased risk of vitamin C deficiency.
- People with type 1 diabetes have increased vitamin C requirements, as do those on hemodialysis and peritoneal dialysis.
- Because vitamin C is absorbed in the small intestine, people with the disease of the small intestine such as Crohn, Whipple, and celiac disease are at risk.
- Iron overload disorders may lead to renal vitamin C wasting.
Pathophysiology
Vitamin C is functionally most relevant for the triple-helix formation of collagen; a vitamin C deficiency results in impaired collagen synthesis. Proline and lysine hydroxylases are required for the post-synthetic modification of procollagen to collagen. Vitamin C is necessary as a coenzyme for these hydroxylases.
Formation of intercellular cement substances in connective tissues, bones, and dentin is defective, resulting in weakened capillaries with subsequent hemorrhage and defects in bone and related structures. Hemorrhaging is a hallmark feature of scurvy and can occur in any organ. Hair follicles are one of the common sites of cutaneous bleeding.
Bone tissue formation becomes impaired, which, in children, causes bone lesions and poor bone growth. Fibrous tissue forms between the diaphysis and the epiphysis and costochondral junctions enlarge. Densely calcified fragments of cartilage are embedded in the fibrous tissue. Subperiosteal hemorrhages, sometimes due to small fractures, may occur in children or adults.
Clinical Manifestations
- Early symptoms are malaise and lethargy.
- After 1-3 months, patients develop shortness of breath and bone pain.
- Myalgias may occur because of reduced carnitine production.
- Other symptoms include skin changes with roughness, easy bruising and petechiae, gum disease(figure-1), loosening of teeth, poor wound healing, and emotional changes.

Figure-1- showing bleeding gums
- Dry mouth and dry eyes similar to Sjögren syndrome may occur.
- In the late stages, jaundice, generalized edema, oliguria, neuropathy, fever, and convulsions can be seen.
- Vital signs: Hypotension may be observed late in the disease. This may be due to an inability of the resistance vessels to constrict in response to adrenergic stimuli.
- Skin: Perifollicular hemorrhages (figure-2), purpura, and ecchymoses are seen most commonly on the legs and buttocks where hydrostatic pressure is the greatest. Poor wound healing and breakdown of old scars may be seen.
- Nails: Splinter hemorrhages may occur.

Figure- 2- showing hemorrhages in the nail bed
- Head and neck: Gum swelling, friability, bleeding, and infection with loose teeth; mucosal petechiae; scleral icterus (late, probably secondary to hemolysis); and pale conjunctiva are seen. Conjunctival hemorrhage, flame-shaped hemorrhages, and cotton-wool spots may be seen. Bleeding into the periorbital area, eyelids, and retrobulbar space also can be seen. Alopecia may occur secondary to reduced disulfide bonding.
- Chest and cardiovascular: Scorbutic rosary (ie, sternum sinks inward) may occur in children. High-output heart failure due to anemia can be observed. Bleeding into the myocardium and pericardial space has been reported.

Figure-3- showing scorbutic rosary
- Extremities: Fractures, dislocations, and tenderness of bones are common in children. Bleeding into muscles and joints may be seen. Edema may occur late in the disease.
- Gastrointestinal: Loss of weight secondary to anorexia is common.
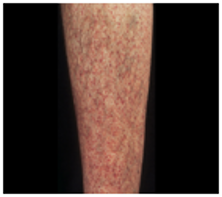
Figure-4- showing perifollicular hemorrhages
Diagnosis
Diagnosis is usually made clinically in a patient who has skin or gingival signs and is at risk of a vitamin C deficiency
Laboratory Investigations
A plasma or leukocyte vitamin C level can confirm the clinical diagnosis.
- Scurvy occurs at levels generally less than 0.1 mg/dL.
- Symptoms occur at levels below 2.5 mg/L, which is considered a deficiency.
- Levels of 2.5-5 mg/L indicate depletion.
- Levels can be low in patients who have tuberculosis, rheumatic fever, or other chronic illnesses; those who smoke cigarettes; and patients on oral contraceptive drugs.
- Capillary fragility can be checked by inflating a blood pressure cuff and looking for petechiae on the forearm.
- Bleeding time, clotting time and Prothrombin time are normal.
- An iron deficiency anemia is generally observed.
Imaging Studies
Skeletal x-rays can help diagnose childhood (but not adult) scurvy. Changes are most evident at the ends of long bones, particularly at the knee.
- Early changes resemble atrophy.
- The loss of trabeculae results in a ground-glass appearance.
- The cortex thins.
- A line of calcified, irregular cartilage(white line of Fraenkel) may be visible at the metaphysis.
- The epiphysis may be compressed.
- Healing subperiosteal hemorrhages may elevate and calcify the periosteum.
Differential Diagnosis
In adults, scurvy must be differentiated from arthritis, hemorrhagic disorders, gingivitis, and protein-energy malnutrition.
Treatment
Patients should take ascorbic acid at 100mg 3-5 times a day until a total of 4 g is reached, and then they should decrease intake to 100 mg daily.
Alternately, ascorbic acid may be taken at 1 g/d for the first 3-5 days followed by 300-500 mg/d for a week. Then the recommended daily allowance is resumed.
- Divided doses are given because intestinal absorption is limited to 100 mg at one time.
- Parenteral doses are necessary for those with gastrointestinal malabsorption.
Diet
Foods high in vitamin C include the following.
- Citrus fruits, especially grapefruits and lemons
- Vegetables, including broccoli, green peppers, tomatoes, potatoes, and cabbage
- The recommended daily allowance for vitamin C varies. The current recommendation for adults is 120 mg daily, although a dose of 60 mg daily is all that is required to prevent scurvy.
- Diets high in vitamin C have been claimed to lower the incidence of certain cancers, particularly esophageal and gastric cancers.
Toxicity
Taking>2 g of vitamin C in a single dose may result in abdominal pain, diarrhea, and nausea. Since vitamin C may be metabolized to oxalate, it is feared that chronic, high-dose vitamin C supplementation could result in an increased prevalence of kidney stones. Thus, it is reasonable to advise patients with a past history of kidney stones to not take large doses of vitamin C. There is also an unproven but possible risk that chronic high doses of vitamin C could promote iron overload in patients taking supplemental iron.