
Search Your Topic
Case study- HIV Infection
Case details
A- 29 years old officer presented to the emergency department complaining of chills and breathing difficulty. He was a heroin abuser who was admitted to the same hospital 7 years ago because of drug overdosage. He had lost 10 kg of body weight since his last clinical visit.
On examination, he had multiple enlarged lymph nodes. Several red nodules were there on the chest and arms. His body temperature was 40oC, B.P. 170/50 mm Hg and respiration were shallow with a respiratory rate of 40 breaths per minute. The chest radiograph showed diffuse pneumonia.
Sputum smear revealed numerous Pneumocystis organisms while skin biopsy revealed Kaposi’s sarcoma.
What is your presumptive diagnosis for this patient?
What is the biochemical basis for all the clinical manifestations seen in this patient?
How can the diagnosis be confirmed?
Case discussion
The patient is suffering from HIV Infection. Intravenous drug usage seems to be the major causative factor. The patient‘s immune system has been collapsed to the extent of loss of resistance to ordinary viral, fungal and protozoal infections which could otherwise have been controlled easily. Kaposi sarcoma and Pneumocystis pneumonia are considered markers of AIDS since they signify the underlying collapsed immune system. Non-specific Fever and weight loss of more than 10% of body weight are also diagnostic of AIDS.
AIDS
Acquired Immunodeficiency Syndrome or AIDS, is a collection of symptoms due to underlying infections and malignancies resulting from the specific damage to the immune system caused by the human immunodeficiency virus (HIV).
Incidence
HIV (human immunodeficiency virus) infection has now spread to every country in the world. Approximately 40 million people are currently living with HIV infection, and an estimated 25 million have died from this disease. The scourge of HIV has been particularly devastating in sub-Saharan Africa, but the infection rates in other countries remain high. In the United States, approximately 1 million people are currently infected.
The first indication of this new syndrome came in 1981 in homosexual drug addict males; they had two things in common- Pneumocystis pneumonia and Kaposi’s sarcoma. Both these are markers of the collapsed immune system, The affected patients appeared to have lost their immune competence, rendering them vulnerable to overwhelming and fatal infections with relatively avirulent micro-organisms, as well as to lymphoid and other malignancies. This condition was given the name Acquired Immunodeficiency Syndrome (AIDS).
In 1986, The International Committee on virus Nomenclature decided on the generic name of the causative virus as the Human Immunodeficiency Virus.
Human Immunodeficiency Virus
HIV, the etiological agent of AIDS, belongs to the lentivirus subgroup of the retroviridae family. This family of viruses is known for latency, persistent viremia, infection of the nervous system, and weak host immune responses. HIV has a high affinity for CD4 T lymphocytes and monocytes. HIV binds to CD4 cells and becomes internalized. The virus replicates itself by generating a DNA copy by reverse transcriptase. Viral DNA becomes incorporated into the host DNA, enabling further replication. Besides HIV, the related animal immunodeficiency viruses are also assigned to this group.
Structural Characteristics of HIV
HIV is a spherical enveloped virus of about 90-120 nm in diameter. (See Figure-1 below). There is a lipoprotein envelop, which consists of lipids derived from the host cell membrane and glycoproteins which are viral coded. The major virus coded envelop proteins are the projecting knob like spikes on the surface and the anchoring transmembrane pedicles. The spikes, gp 120 constitute the major surface component of the virus which binds to the cell CD4 receptors on susceptible host cells. These specific receptors, known as cluster of differentiation- CD4 are present on certain cells in the body, the cells possessing these receptors are called CD 4 + cells and these are -T helper cells, B lymphocytes, macrophages, monocytes, and dendritic cells. Transmembrane pedicles gp 41 cause cell to cell fusion.
Interior to the envelope is an outer icosahedral nuclear capsid shell and an inner cone-shaped core containing ribonucleoproteins. The enzymes integrase p32, protease p10, reverse transcriptase p55/66 and 2 copies of single-stranded genomic RNA are present inside the core. (The proteins and glycoproteins are indicated by their mass expressed as kilo Daltons)
The reverse transcriptase enzyme is a characteristic feature of retroviruses. When the virus infects a cell, the viral RNA is transcribed by the enzyme first into single-stranded DNA and then into double-stranded DNA (provirus), which is integrated into the host cell chromosome. The provirus can remain latent for a long period though it influences the host cell functions. At times in response to viral promoters, the provirus initiates viral replication by directing the synthesis of viral RNA and other components.

Figure-1-A cross-sectional schematic diagram of HIV virion, showing lipid bilayer in the form of the viral envelope, Nucleocapsid core, which includes a layer of a protein called p17 and an inner layer of a protein called p24. The HIV genome consists of two copies of the single-stranded RNA, which are associated with two molecules of Reverse transcriptase p64, protease p10, and integrase p32. The outer viral proteins are gp 120 and gp 41.
Genome of HIV
There are two types of genes analyzed, (See figure-2)
a) Structural genes encode for products which participate in the formation of a functional structure of virus-
1) gag gene – encodes for core and shell of the virus. The gene product is a precursor protein p55, which is cleaved into p17, p24, and p15. The p24 antigen (major core antigen) can be detected in serum during the early stages of infection until the appearance of the antibodies.
2) pol gene– encodes for the polymerase reverse transcriptase and other viral enzymes such as protease and integrase. It is expressed as a precursor protein, which is cleaved into components like p64 which has reverse transcriptase and RNAse activity: p51 which has only reverse transcriptase activity: p10 is a protease that cleaves gag precursor and p32 is an integrase.
3) env gene – determines the synthesis of envelop glycoprotein gp 160 which is cleaved into gp 120 and gp 41. Glycosylation occurs after cleavage. The antibodies to gp 120 are the first to appear after HIV infection and are present in circulation till the terminal stage of infection.
b) Non-structural and Regulatory genes
1) vif (Viral infectivity factor gene) influences the infectivity of viral particles.
2) vpr–stimulates promoter region of the virus
3) vpu (only in HIV-1) and vpx(only in HIV-2) enhance maturation and release of progeny virus from cells. Detection of the type-specific sequences vpu and vpx is useful in distinguishing between infection by HIV type 1 and 2.
4) tat – (transactivating gene) – (2 copies) having a stimulatory effect on synthesis of all viral proteins.
5) rev – (Regulator of viral genes) – (2 copies)–required for expression of structural genes.
6) nef (negative factor gene) downregulates viral replication. It may be responsible for the regulation of the latent state of the virus.
7) LTR – (long terminal repeat) sequences flanking on both sides giving promoter, enhancer and integration signals.

Figure-2 schematic representation of the HIV genome
Antigenic variations in HIV
Based on molecular and antigenic differences, two types of HIV have been recognized. The original isolates of HIV and the related strains present all over the world belong to HIV type 1. The HIV strains, first isolated from West Africa, which react with HIV type I antiserum very weakly or not at all have been termed as HIV type 2. It has a 40 % genetic similarity and is more closely related to the Simian immunodeficiency virus than to HIV-1. It can cause AIDS but is less pathogenic and is less common. It infects mainly monkeys and other similar species and is largely confined to West Africa, though isolations have been reported from some other areas, including Western and Southern India. The envelope antigens of the two types are different though their core peptides show some cross-reactivity.
HIV is a highly mutable virus and exhibits frequent antigenic variations as well as differences in other features such as nucleotide sequences, cell tropism, growth characteristics, and cytopathology. Not only are there differences between isolates of HIV from different races or persons but also between sequential isolates from the same person and even between those obtained from different sites of the same person at the same time. This great variability is believed to be due to the error-prone nature of reverse transcription. Antigenic variation is most frequent in respect of the envelope proteins but is also seen with other antigens.
HIV-1 strains have been classified into at least ten subtypes base on sequence analysis of their gag and env genes. These subtypes have been are designated as A to J and constitute the Group M (For major), which causes the large majority of HIV-1 infections worldwide. A few HIV-1 strains isolated from West Africa do not fall within the major group and have been designated as group O ( For Outlier) Some later isolates of HIV-1 distinct from M and O groups have been called Group N (for new)
Modes of transmission
HIV is transmitted when the virus enters the body, usually by injecting infected cells or semen. There are several possible ways in which the virus can enter.
1) Sexual contact- In 75 % of cases, the transmission is by sexual contact. Most commonly, HIV infection is spread by having sex with an infected partner. The virus can enter the body through the lining of the vagina, vulva, penis, rectum, or mouth during sex. People who already have a sexually transmitted disease, such as syphilis, genital herpes, chlamydia infection, gonorrhea, or bacterial virginities, are more likely to acquire HIV infection during sex with an infected partner.
2) Parenteral- In 15 % cases, it is by blood transfusion or blood product transfusion. Blood products are now tested to minimize this risk. Sharing of unsterilized needles or syringes in drug addicts contaminated with blood from an infected person can also spread the virus. HIV can be spread in health-care settings through accidental needle sticks or contact with contaminated fluids. HIV can also spread through organ transplantation. If tissues or organs from an infected person are transplanted, the recipient may acquire HIV. Donors are now tested for HIV to minimize this risk.
3) From mother to child: Women can transmit HIV to their babies during pregnancy or birth when infected maternal cells enter the baby’s circulation.30% of children born to infected mothers have the acquired infection unless the virus is treated by antiviral drugs before pregnancy. In nursing, the mother’s transmission can occur through breast milk.
Mortality/Morbidity
The course of HIV infection is characterized primarily by latency. Unfortunately, profound immune suppression eventually develops and the illness appears to be almost uniformly lethal. More than 500,000 persons have died of AIDS in the United States.
Progression from HIV infection to AIDS occurs 8-10 years after infection without antiretroviral treatment. In the recent past, most patients would not survive more than 1-2 years following the diagnosis of AIDS. However, since the introduction of highly active antiretroviral therapy (HAART) and prophylaxis against opportunistic pathogens, death rates from AIDS have declined significantly. An HIV-positive patient older than 50 years with a nearly undetectable viral load and a CD4 count more than 350 now has less than a 5% chance of dying or progressing to full-blown AIDS within 3 years.
Age
Most AIDS cases occur in adults aged 25-49 years (70% of cases). Adolescents and young adults (aged 13-24 y) represent 25% of new cases. Young children represent less than 1% of AIDS cases in the United States. Internationally, children younger than 15 years are estimated to account for close to 10% of all HIV cases.
Pathogenesis
Infection is transmitted when the virus enters the blood or tissues of a person and comes in to contact with a suitable host cell, principally the CD4 lymphocytes. The virus may infect any cell bearing the CD4 antigen on the surface. Primarily these are the CD4 + helper T lymphocytes. Some other immune cells possessing CD4 antigens are also susceptible to infection, like B lymphocytes, monocytes, and macrophages including specialized macrophages such as Alveolar macrophages in the lungs and Langerhans cells in the dermis. Glial cells and microglia cells are also susceptible. Follicular dendritic cells from tonsils can be infected by HIV without the involvement of CD4. The steps of viral entry into the host cell are as follows-
- Attachment of virus into the host cell–Specific binding of the virus to the CD4 receptors is by the envelope glycoprotein gp120.
- Cell to cell fusion –For infection to take place the cell fusion is essential. This is brought about by the transmembrane glycoprotein gp 41. HIV-1 utilizes two major co-receptors along with CD4 to bind to, fuse with, and enter target cells; these co-receptors are CCR5 and CXCR4, which are also receptors for certain endogenous chemokines. Strains of HIV that utilize CCR5 as a co-receptor are referred to as macrophage-tropic viruses. Strains of HIV that utilize CXCR4 are referred to as T cell- tropic viruses. Many virus strains are dual tropic in that they utilize both CCR5 and CXCR4.
The infected CD4 cells express a high level of gp 120 on their surface. The gp 120 on the surface of infected cells leads to the fusion of these cells with CD4 protein of uninfected neighboring cells with the formation of multinucleated syncytial cells. The lysis of fused cells finally occurs resulting in depletion of a large number of uninfected cells from the circulation.
- Uncoating of the viral envelope and entry of nuclear capsid core into the cell –After fusion of the virus with the host cell membrane, the HIV genome is uncoated and internalized into the cell. Viral RNA is released into the core cytoplasm.
- Viral transcription– viral reverse transcriptase mediates transcription of its RNA; RNA-DNA hybrid is formed. The original RNA strand is degraded by ribonuclease H, followed by synthesis of the second strand of DNA to yield double-stranded HIV DNA
- Integration into the host DNA as provirus- The double-stranded DNA is integrated into the genome of the infected host cell through the action of the viral integrase enzyme, causing a latent infection.
- The fate of provirus-From time to time, lytic infection is initiated by releasing progeny virions, which infect other cells. The long and variable incubation period of HIV is because of the latency. In an infected individual, the virus can be isolated from the blood, lymphocytes, cell-free plasma, semen, cervical secretions, saliva, urine, and breast milk.
- Transcription back into RNA – The viral DNA is transcribed into RNA and multiple copies of viral RNA are produced. There are only nine genes in HIV RNA and these code for the production of structural proteins, accessory proteins, and enzymes essential for the virus’s replicative cycle.
- Virion assembly – With the help of viral protease, the new virions are assembled into the polypeptide sequences needed for HIV virion formation and infectivity.
- Cell lysis. The infected cell is made to burst open, presumably by the action of cellular proteins. (See figure-3)

Figure-3 showing the life cycle of HIV (Integration and excision of viral genome)
Causes of immunodeficiency
The primary pathogenic mechanism in HIV infection is the damage caused to the CD4+ T lymphocytes- The T4 cells decrease in numbers and the T4: T8 cell ratio is reversed. The infected cells do not release cytokines. This has a marked damping effect in the cell-mediated immune response. Though the major damage is to cellular immunity, the humoral mechanisms are also affected. AIDS patients are unable to respond to new antigens. There is polyclonal activation of B lymphocytes leading to Hypergammaglobulinemia. These are nonspecific antibodies and are irrelevant to antigens.
Monocyte, macrophage system is also affected apparently due to the lack of the activating factors by the T4 lymphocytes. The activity of NK cells and Tc (T Cytotoxic) cells are also affected. The clinical manifestations are due to the failure of the immune responses. This renders the patient susceptible to life-threatening opportunistic infections and malignancies. The exceptions to this may be the neurological lesions seen in AIDS. Dementia and other degenerative neurological lesions seen in AIDS are due to the direct toxic effects of HIV on the central nervous system.
Clinical Manifestations
AIDS is only the last stage in the wide spectrum of clinical features in HIV infection. The center for disease control (USA) has classified the clinical course of HIV infection under various groups.
- Acute HIV infection
- Asymptomatic or Latent infection
- Persistent generalized lymphadenopathy (PGL)
- AIDS-related complex
- Full-blown AIDS (Last stage)
- Acute HIV infection
Many people do not develop symptoms after they first get infected with HIV. Others have a flu-like illness with fever, sore throat, headache, tiredness, skin rashes and enlarged lymph nodes in the neck within several days to weeks after exposure to the virus. These symptoms usually disappear of their own within a few weeks. The test for HIV antibodies appears negative while HIV antigenemia (p24 antigen) and viral nucleic acids can be demonstrated at the beginning of the phase. This phase is also called window period or phase of Seroconversion.
2) Asymptomatic or Latent infection
All persons infected with HIV, pass through a phase of symptomless infection (Clinical latency), which may last up to several years. The progression of the disease varies widely among individuals. This state may last from a few months to more than 10 years. During this period, the virus continues to multiply actively and infects and kills the cells of the immune system. The virus destroys the CD4 cells that are the primary infection fighters.
Even though the person has no symptoms, he or she is contagious and can pass HIV to others through the routes listed above. The patients show positive antibody tests during this phase. The infection progresses in course of time through various stages, CD4 lymphocytopenia, minor opportunistic infections, persistent generalized lymphadenopathy, AIDS-related complex, ultimately terminating in full-blown AIDS.(Figure-5) The median time between primary HIV infection and the development of AIDS has been stated as approximately 10 years. About 5-10 % percent of the infected appear to escape clinical AIDS for 15 years or more. They have been ‘long term survivors” or “long term nonprogressors”. The mechanism for such long time survivors is not exactly known, though many viral and host determinants are responsible.
During this period the host mounts an immune response against the virus, both humoral and cellular, which can only limit the viral load but cannot clear it completely. Chronic persistent infection with varying degree of multiplication is the result.
3) Persistent generalized lymphadenopathy (PGL)
This has been defined by the presence of enlarged lymph nodes, at least I cm in diameter, in two or more noncontiguous extra inguinal sites, that persist for at least three months, in the absence of any current illness or medication that may cause lymphadenopathy. These are diagnostic of HIV when blood tests are positive for antibodies.
4) AIDS-related complex
This group includes patients with considerable Immunodeficiency suffering from various constitutional symptoms of minor opportunistic infections. The patients present with weight loss – of more than 10% of body weight, persistent fever, diarrhea, generalized fatigue and signs of other opportunistic infections may be apparent. The opportunistic infections are oral candidiasis, herpes zoster, salmonellosis or Tuberculosis, and hairy cell leukoplakia. The patients are usually severely ill and many of them progress to AIDS in a few months. The CD4 cell count decreases steadily when the count falls to 200, or less, clinical AIDS usually sets in. For this reason, the case definition by CDC includes all HIV infected cases with CD4 + T cell counts of 200 or less, irrespective of the clinical condition.
5) Full-blown AIDS
This is the end stage disease representing the irreversible break down of immune defense mechanisms. In addition to opportunistic infections, the patient may develop primary CNS lymphomas and progressive multifocal leukoencephalopathy, dementia and other neurological abnormalities. Kaposi sarcoma (Figure-4) and Pneumocystis pneumonia are almost always observed in a majority of patients.

Figure- 4-showing Kaposi’s sarcoma- it is an indolent, multifocal non metastasizing mucosal or cutaneous tumor probably of endothelial origin, represented in the form of purple spots in the skin.

Figure-5 showing the disease progression through different phases in HIV infected cases.CD4 count comes down while the viral count goes high with the passage of time.
Laboratory Diagnosis of HIV infection
Laboratory procedures for the diagnosis of HIV infection include tests for immunodeficiency as well as specific tests for HIV.
1) Non Specific Tests– The following tests help to establish the immunodeficiency in HIV infection.
a) Total Leukocyte and lymphocyte count- to demonstrate leucopenia and lymphopenia. The lymphocytic count is usually below 2000/mm3
b) T cell subset Assays- Absolute CD4+ cell count is less than 200 /L.T4 T8 ratio is reversed. The decrease in CD4 is the hall-mark for AIDS.
c) Platelet count– shows Thrombocytopenia.
d) IgA and IgG levels are raised
e) Diminished cell-mediated Immunity as indicated by skin tests
f) Lymph node biopsy shows profound abnormalities.
2. Specific Tests for HIV infection- These include the demonstration of HIV antigen, antibodies. Viral nucleic acids or other components and isolation of virus-
i) Detection of antigen-Following a contact, as by blood transfusion, the viral antigen may be detectable in the blood after about 2 weeks. The major core antigen p24 is the earliest virus marker to appear in the blood. IgM antibodies appear in about 4-6 weeks, to be followed by IgG antibodies
If the infecting dose is small, as following a needle stick injury, the process may be considerably delayed. Afterward, free p24 antigen disappears from circulation and remains absent during the long asymptomatic phase to reappear only when severe clinical disease sets in. However, antibody-bound p24 antigen continues to be demonstrable, after dissociation.
The p24 Capture ELISA assay, which uses anti p24 antibody as the solid phase can be used for this. This test is positive in about 30% of the infected persons. In the first few weeks after infection and in the terminal phase, the test is uniformly positive. This test along with HIV ELISA is currently used for screening blood donors.
ii) Detection of antibodies
Demonstration of antibodies is the simplest and most widely employed technique for the diagnosis of HIV infection. However, it takes 2-8 weeks to months for the antibodies to appear in circulation and during that period the person may be highly infectious. Once antibodies appear they increase in titer for the next several months. IgM antibodies disappear in 8-10weeks while IgG antibodies remain throughout. When immunodeficiency becomes severe following clinical AIDS some components of anti p24 may disappear. There are two types of serological tests- Screening tests and supplemental tests.
i) Screening tests include-
ELISA- ELISA is the most frequently used method for screening of blood samples for HIV antibody. The sensitivity and specificity of the presently available commercial systems approach 100% but false positive and false negative reactions occur.
1) First-generation – whole viral lysates
2) Second generation – recombinant antigen
3) Third generation – synthetic peptide
4) Fourth-generation – antigen + antibody (Simultaneous detection of HIV antigen and antibody) – HIV duo
The antibody can be detected in a majority of individuals within 6-12 weeks after infection using the earlier generation of assays. But it can be detected within 3-4 weeks when using the newer third-generation ELISA. Due to their ability to detect p24 antigen, the fourth-generation ELISA will be of value in detecting early infection. The window period can be shortened to two weeks using the p24-antigen assay.
ii) Supplemental Tests
a) Western Blot Test
b) Indirect Immunofluorescence test
c) Radio Immunoprecipitation Assay
iii) Rapid Tests
a) Dot Blot assay
b) Particle Agglutination tests
c) HIV spot and comb test
d) Fluorimetric microparticle technologies
Western blotting- Western blots are regarded as the gold standard and seropositivity is diagnosed when antibodies against both the env and the gag proteins are detected. The sensitivity of the test systems is currently being improved by the use of recombinant antigens.
Rapid tests- These are tests that can yield results in < 30 min. The results are read by the naked eye.
Rapid HIV assays have proven particularly useful for testing pregnant women in labor who have not received prenatal care. These are also helpful in detecting HIV-2 infection which cannot be detected by ELISA.
3) Demonstration of viral Nucleic acid – this can be accomplished by probes or by PCR techniques. The latter may be useful because of its extremely high sensitivity. Although standard tests that measure antibody response to the HIV virus have become increasingly sensitive, cases of HIV are occasionally missed because individuals can have negative antibody tests during the early stages of infection. Also, a few people with long-term HIV infection may have false-negative antibody tests or maybe chronic carriers who are clinically asymptomatic.
PCR -In this, the target HIV RNA or proviral DNA is amplified enzymatically in vitro by chemical reaction. It is an extremely sensitive assay because a single copy of proviral DNA can be amplified. Qualitative PCR is useful for diagnostic purposes.
Three different techniques namely RT-PCR, nucleic acid sequence-based amplification (NASBA) and branched-DNA (b-DNA) assay have been employed to develop commercial kits.
4) Virus isolation– virus isolation is accomplished by the co-cultivation of the patient’s lymphocytes with fresh peripheral blood cells of healthy donors or with suitable culture lines such as T-lymphomas. The presence of the virus can be confirmed by reverse transcriptase assays, serological tests, or by changes in the growth pattern of the indicator cells. However, virus isolation is tedious and time-consuming (weeks) and is successful in only 70 to 90% of cases. Therefore virus isolation is mainly used for the characterization of the virus.
5) Alternative to classical tests
a) Oral fluid (saliva) HIV tests
b) Urine tests
Treatment
Virtually all treatment for HIV infection and AIDS today focuses on arresting the progression of the disease within the body as measured by T cell counts and tests for viral load.
At present, a reasonable course of action is to initiate ARV( Antiretroviral)therapy in anyone with the acute HIV syndrome; all pregnant women; patients with symptomatic disease; and patients with the asymptomatic disease with CD4+ T cell counts <350/L. In addition, one may wish to administer a 6-week course of therapy to uninfected individuals immediately following a high-risk exposure to HIV.
There are two principal approaches to treatment: immunotherapy and anti-HIV drug treatments
a) Immunotherapy– Immunotherapy is transfusion based treatment designed to replace lost immunoglobulins needed to fight HIV infection (passive immunotherapy), to provide cellular factors such as interleukins (IL-2) or to introduce selected or altered immune cells to attack cells harboring the virus (adoptive immunotherapy). The results of trials using this latter approach, however, have been inconclusive, and no group has yet shown a survival benefit.
b) Anti-HIV drug treatment-Treatment with anti-HIV drugs attempts to reduce the viral load by blocking new infection in the host cell. The drugs used to target two major enzymes of HIV which are needed for the infection cycle: reverse transcriptase and protease.
I) Reverse transcriptase inhibitors– Reverse transcriptase inhibitors act at the pre-integration stage – before the viral RNA has been converted to DNA and enters the host cell nucleus to integrate into the cell chromosome. These drugs block the reverse transcription of viral RNA into viral DNA. There are two types of reverse transcriptase inhibitors, both of which accomplish the same objective: nucleoside and nucleotide analogs, and non-nucleoside reverse transcriptase inhibitors.
i) Nucleoside analogs, which constitute the most effective family of antiretroviral drugs, operate by mimicking nucleic acids normally incorporated into viral DNA. They interfere with reverse transcriptase and thus prevent infection. Nucleoside analogs can be placed in two groups, those replacing thymidine, such as AZT and d4T, which protect activated T cells from infection, and non-thymidine analogs such as ddI and 3TC, which protect resting T cells.
Nucleotide analogs have the same action but are based around a different sugar.
ii) Non-nucleoside reverse transcriptase inhibitors directly inhibit reverse transcription and, unlike nucleoside analogs, do not have to go through chemical changes in the infected cell before beginning their action. The two main non-nucleoside reverse transcriptase inhibitors are nevirapine, which can show toxicity and early resistance problems, and delavirdine, with which there is a less clinical experience as yet.
2) Protease inhibitors –Protease inhibitors block HIV replication after integration. These drugs inhibit the function of the protease by acting as analogs for the peptide and non-peptide protease substrates needed to process the ‘gag-pol’ polypeptide into proteins. As a result, no infectious virus can be produced.
Since protease inhibitors act after integration, they can obstruct infectious HIV production in both acutely and chronically infected T cells and macrophages. (In contrast, reverse transcriptase inhibitors can only inhibit the acute infection of cells.). Protease inhibitors have also been shown to be less toxic than nucleoside analogs. So far only a few have been licensed for use, including saquinavir, ritonavir, indinavir, and, more recently, nelfinavir, although others are expected. (Figure-6)
3) Combination treatment -Because reverse transcriptase inhibitors and protease inhibitors address different stages of viral replication, using both families of drugs in combination has been shown to be more effective than monotherapy in impeding the spread of HIV in the body and reducing viral loads. Although the optimum combination of anti-HIV drugs is as yet unknown, AZT, 3TC, and a protease inhibitor are usually the first drugs given. This combination of two reverse transcriptase inhibitors, one of which is a thymidine analog, and a protease inhibitor, blocks infection both before and after integration and in both activated and resting T cells. The aim of anti-HIV therapy has now shifted from simply delaying the progression of the disease to finding a permanent cure. This combinational therapy is termed as highly active antiretroviral therapy (HAART).
The current consensus is that one should give a potent combination of agents, HAART right from the start when treatment is indicated.
4) The future- In addition to the positive results shown by combination therapy trials, a number of developments may hold promise for the near future. These include genetically engineered killer T cells that attack HIV before it reproduces, and research into genetically deactivating the CXCR4 and CCR5 T cell co-receptors, which are a path for HIV entry into cells.
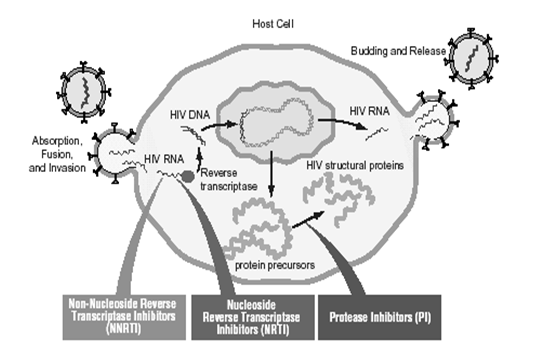
Figure-6 showing the mechanism of action of different drugs used for the treatment of HIV infection
Prevention
The risk of contracting HIV increases with the number of sexual partners. A change in lifestyle would obviously reduce the risk.
HIV-infected mothers are not recommended to have children at present and pregnancy itself would appear to be a risk factor for seropositive mothers. A recent clinical trial demonstrated the efficacy of AZT in preventing transmission of HIV from the mother to the fetus.
The spread of HIV through blood transfusion had virtually been eliminated since the introduction of blood donor screening in many countries. Blood products such as factor VIII now undergo routine treatment which appears to inactivate any HIV present effectively.
Development of vaccine
The development of a vaccine is fraught with several problems unique to this virus. These include-
1) HIV can mutate rapidly, thus, it is not possible to design antibodies against all antigens.
2) Antibody alone is not sufficient, cell-mediated immunity may also be necessary.
3) The virus enters the body not as free virions but also as infected cells, in which the virus or the provirus is protected against antibody or cell-mediated lysis.
4) Virus readily establishes lifelong latent infection hiding from antibodies.
The main types of approaches to an AIDS vaccine are as follows:
- Live attenuated virus
- Inactivated virus
- Live recombinant viruses
- Synthetic peptides
- Recombinant DNA products (gp120, gp160)
- Native envelope and/or core proteins
- Anti-idiotypes antibodies
- Passive immunization
To date, the best hope lies in an inactivated vaccine
Despite progress in dealing directly with HIV, however, the virus, by impairing the immune system, exposes the infected person to a range of opportunistic viral, bacterial, and parasitic infections and malignancies. It is these which are the actual cause of death in most patients with AIDS, it is still unclear whether HIV induced damage to the immune system can be reversed. New strains of HIV undetectable by current screening methods and resistant to the best antiretroviral drugs currently available have also now been discovered.